Social and Emotional Development In Child-Care Settings
A significant proportion of children spend at least some time in non-parental care during their first five years of life. This chapter focuses on aspects of non-parental care that shape the development of social and emotional competencies in young children (Figure 4.1).
Similar to parent-child interactions, interactions that children have with non-parental caregivers can play an important role in promoting child development. This may be driven by the education level and training of the provider, as well as the overall quality of the non-parental care. The types of child care, including center-based, family child-care homes, relative care, or care in the home by a nonrelative — differ in their level of formality, the way they are set up, and the qualifications of the caregivers. This suggests that there may be unique needs for each setting to ensure that all children in Shelby County are receiving care in a way that maximizes their social and emotional development.
We focus much of the discussion in this chapter on formal (typically licensed) child-care providers, including center-based and family child care home settings. However, these issues can also apply to informal settings.

Formal child-care providers offer two main types of support important for children’s social and emotional development 40, 41.
- Instructional support provides learning experiences or encourages skill development through interactions between a child and a child-care provider.
- Emotional support, defined by the warmth and sensitivity provided to the child, encourages the development of social and emotional competencies through responsive and supportive interactions 40, 42.
Data facts:
- Nationally, only 13 percent of preschool teachers get high ratings on instructional support 43.
- Nationally, fewer than half of preschool teachers are rated as having a high level of emotional support 43.
Why are provider-child interactions important?
The interactions between children and their child-care providers contribute to the development of children’s emerging social and emotional skills.
Positive provider-child relationships in early childhood often include a high degree of warmth and closeness, a minimal amount of conflict, and can occur when the child is able to share the provider with other children in the group setting 42-45.
Children who are in high-quality formal child care have:
- Increased social skills at the end of the preschool year 42
- Improved academic school readiness 43
- Less problem behavior at school entry and at the beginning of high school 42, 46
- Better academic outcomes, which persist from school entry to the end of high school 46.
Where do children spend their time?
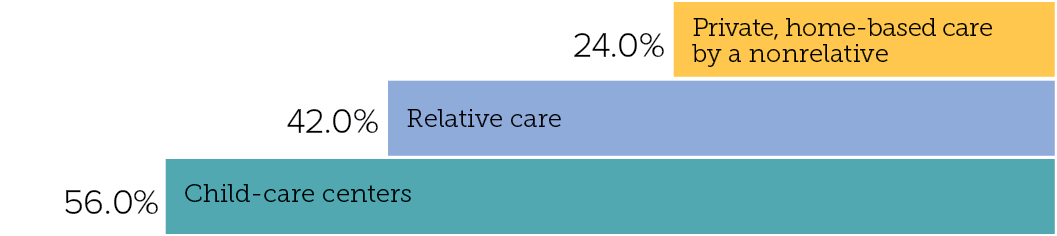
Many children spend a significant amount of time in the care of someone other than their parents or guardians. Nationally, about 60 percent of children ages five and under who are not yet enrolled in school are in some form of non-parental child care on a weekly basis 48, 49 (Figure 4.2).
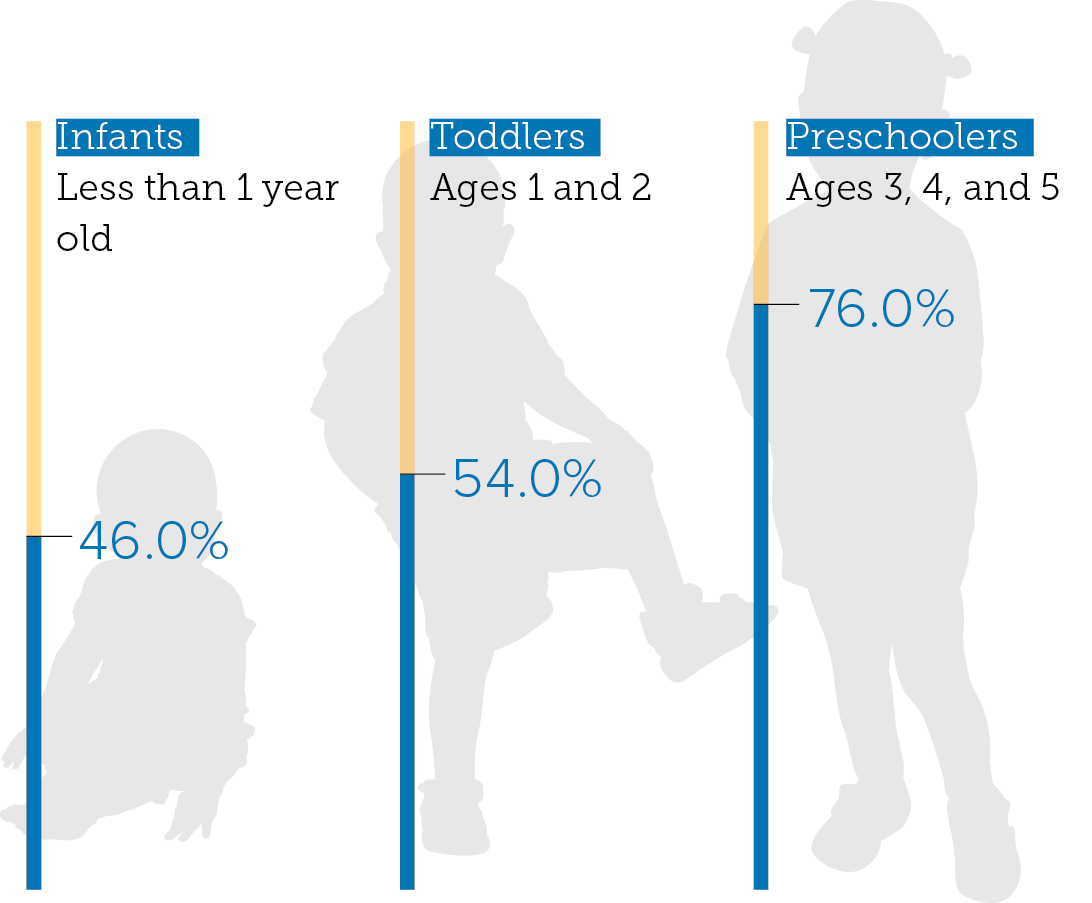
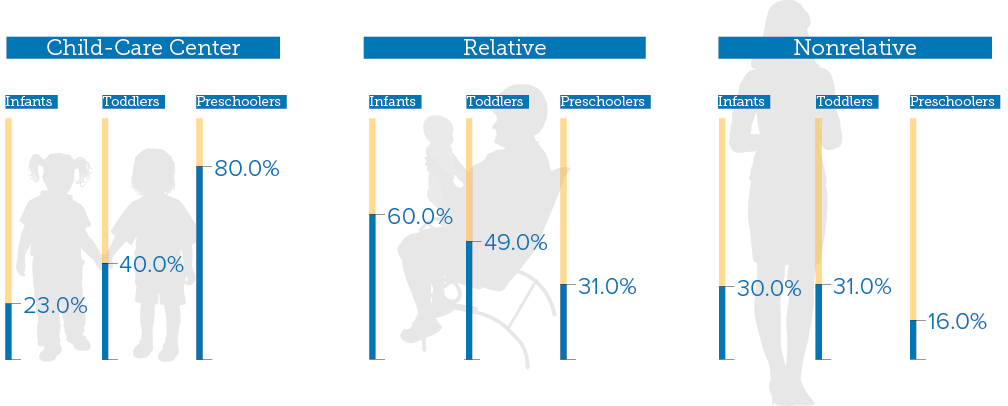
The use of non-parental care and the type of non-parental care most typically used by parents varies by the age of the child (Figure 4.3). Generally, use of care—and more specifically, use of center-based care—is greater for older children, ages 3 and 4 (Figure 4.4). By then, most children are in center-based settings on a regular basis 49.
Data fact:
- Preschool-age children spend about 33 hours per week in child care 48.
What do we know about child-care quality in Shelby County?
Child-care quality is hard to measure in Shelby County because there is not a standard way to assess it. Currently, two programs are used to assess licensed child care quality above minimum licensing requirements: the Tennessee-initiated Star-Quality Child Care Program and National Association for the Education of Young Children (NAEYC) accreditation. Participation in either rating system is voluntary. Although measures of provider-child interactions are not assessed directly as part of the Star-Quality program, higher standards present in three-star providers or NAEYC-accredited centers may be more likely to foster positive provider-child interactions or promote positive social and emotional development. However, more work is needed to validate these rating scales with respect to social and emotional outcomes of children.

Data facts:
- About 67 percent of eligible Shelby County licensed child-care providers participate in the Star-Quality rating program. Of these, 87 percent of center-based providers have a three-star rating, and 78 percent of family child-care providers have a three-star rating. Table 4.1 shows the distribution of the star ratings among providers who participated.
- In Shelby County, only about 7 percent of all licensed centers are accredited by NAEYC.
Sources: Tennessee Child Care Management System for September 2014, provided by Child Care ReSource and Referral (LeBonheur Community Health and Well Being Division); NAEYC Accredited Program Search, http://www.naeyc.org/academy/accreditation/search
Where are three-star providers located?
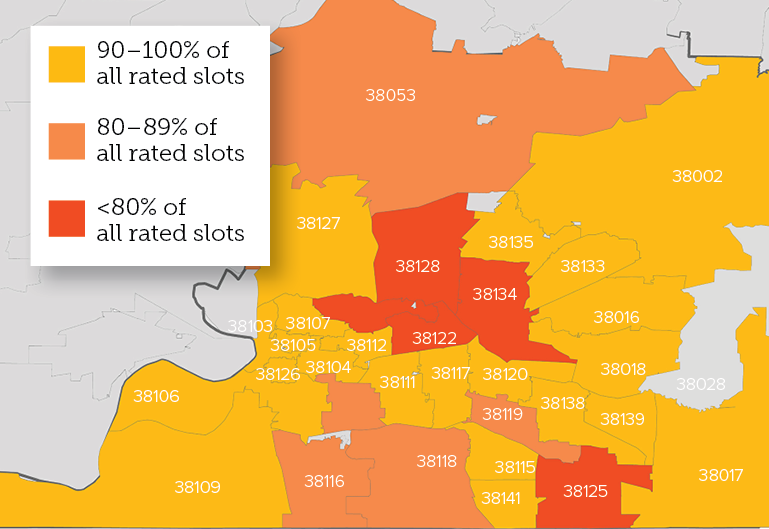
It is helpful to understand the geographic distribution of higher-quality licensed child care across the county to identify areas of need and potential models of success. While this is difficult to assess due to the voluntary nature of the quality rating systems, we can get a glimpse into this by looking at child-care providers who participated in the Star-Quality rating system. The map in Figure 4.5 shows the proportion of child-care slots in each zip code that are in three-star providers. This map does not include child-care providers that did not participate in the Star-Quality rating system, including centers that are NAEYC-accredited but do not have a Star-Quality rating. As a result, it provides a limited look at child-care quality in Shelby County. Zip codes with the lowest proportion of three-star child-care slots include 38122 (54 percent), 38125 (72 percent), 38134 (72 percent), 38108 (78 percent), and 38128 (79 percent).
Conclusion
Children spend a substantial part of their time in non-parental care both inside and outside the home. Because of this, it is important to understand the current state of provider-child interactions that promote social and emotional health. Though little data exist to examine this locally, two quality-rating systems provide some insight. However, these systems have limitations, as well. First, they are voluntary, meaning there is no centralized data to examine child-care quality across Shelby County. Second, the Tennessee Star-Quality program does not explicitly capture provider-child interactions, which we know to be important. Third, they are not used to assess quality of provider-child interactions in more informal settings. Finding ways to improve child-care quality—and our measurement of quality—will increase the number of children who have access to high-quality care in Shelby County.
- La Paro, K.M., Pianta, R.C. , & Stuhlman, M. (2004). The classroom assessment scoring system: Findings from the prekindergarten year. The Elementary School Journal, 104(5), 409–426.
- Pianta, R., Howes, C., Burchinal, M., Bryant, D., Clifford, R., Early, D., & Barbarin, O. (2005). Features of pre-kindergarten programs, classrooms, and teachers: Do they predict observed classroom quality and child-teacher interactions? Applied Developmental Science, 9(3), 144–159.
- Mashburn, A.J., Pianta, R.C., Hamre, B.K., Downer, J.T., Barbarin, O.A., Bryant, D., et al. (2008). Measures of classroom quality in prekindergarten and children’s development of academic, language, and social skills. Child Development, 79(3), 732–749.
- Burchinal, M., Vandergrift, N., Pianta, R., & Mashburn, A. (2010). Threshold analysis of association between child care quality and child outcomes for low-income children in pre-kindergarten programs. Early Childhood Research Quarterly, 25(2), 166–176.
- Howes, C., Burchinal, M., Pianta, R., Bryant, D., Early, D., Clifford, R., et al. (2008). Ready to learn? Children’s pre-academic achievement in pre-kindergarten programs. Early Childhood Research Quarterly, 23(1), 27–50.
- Sabol, T.J., & Pianta, R.C. (2012). Recent trends in research on teacher-child relationships. Attachment & Human Development, 14(3), 213–231.
- Vandell, D.L., Belsky, J., Burchinal, M., Vandergrift, N., & Steinberg, L. (2010). Do effects of early child care extend to age 15 years? Results from the NICHD study of early child care and youth development. Child Development, 81(3), 737–756.
- Hamre, B.K, (2012). A Course on Effective Teacher-Child Interactions Effects on Teacher Beliefs, Knowledge, and Observed Practice. American Education Research Journal, 49(1), 88–123.
- Laughlin, L. (2011). Who’s Minding the Kids?: Child Care Arrangements. U.S. Department of Commerce, Bureau of the Census.
- Mamedova, S., & Redford, J. (2013). Early childhood program participation, from the National Household Education Surveys Program of 2012 (NCES 2013-029). Washington, D.C.: National Center for Education Statistics, Institute of Education Sciences, U.S. Department of Education.